Can Magnetic Fields Help Heal the Brain?
A New Frontier in Brain Health
Imagine lying back in a comfortable chair as gentle pulses of magnetic energy pass silently through your brain—no surgery, no implants, no medication. Just targeted magnetic fields, carefully applied. Over time, your mood begins to lift. Your thinking feels clearer. Memory returns with greater ease.
This isn’t speculative. It’s the emerging science of Transcranial Magnetic Stimulation (TMS)—and, increasingly, related to it, Pulsed Electromagnetic Field (PEMF) therapy. Both approaches work by engaging one of the brain’s most remarkable healing molecules: BDNF (Brain-Derived Neurotrophic Factor).
What is BDNF—and Why Does It Matter?
BDNF can be thought of as fertiliser for the brain. It helps neurons grow, connect, regenerate, and survive. It’s essential for:
- Learning and memory
- Mood regulation
- Cognitive resilience
- Recovery after injury
- Protection from neurodegenerative diseases
Low levels of BDNF have been associated with depression, Alzheimer’s, Parkinson’s disease, multiple sclerosis (MS), and brain fog after trauma. Naturally increasing brain BDNF levels—without invasive procedures or pharmaceuticals—is a meaningful step forward in brain health.
How Magnetic Therapy Supports BDNF
A 2025 study by Yalachkov and Karimi-Abdolrezaee in Frontiers in Neurology found that magnetic stimulation significantly increases BDNF levels in both animals and humans. Here’s how:
- Neural stimulation: Targeting areas like the prefrontal cortex triggers BDNF production.
- Neuroplasticity: Repeated pulses mimic learning and exercise, helping the brain adapt and rewire.
- Immune regulation: Magnetic fields support glial cells and reduce inflammation, aiding recovery.
This isn’t just about “boosting brain power.” It’s also about fostering the brain’s natural capacity to heal.
Who Might Benefit?
Here’s a look at some of the ways how BDNF and magnetic stimulation are showing promise across various conditions:
| Condition | How BDNF Helps |
|---|---|
| Depression | Lifts mood, promotes new neural pathways |
| Alzheimer’s Disease | Supports memory and slows cognitive decline |
| Parkinson’s Disease | Helps dopamine-producing neurons survive |
| Multiple Sclerosis (MS) | Improves mental clarity and reduces fatigue |
| Traumatic Brain Injury | Encourages cognitive recovery and focus |
| Stroke Recovery | Aids in motor relearning and coordination |
The Role of PEMF Therapy
PEMF therapy, while often associated with physical medicine and pain management, is now being explored for its neurological benefits. Though research into brain-specific outcomes is still evolving in early stages, initial findings suggest PEMF can may:
- Improve mood and sleep
- Reduce neuroinflammation
- Enhance circulation and cellular repair
- Enhance cognitive function
PEMF offers a non-invasive, drug-free approach that can complement other therapeutic strategies. When delivered with appropriate intensity and consistency, it has the potential to become a valuable part of long-term neurological care.
Why Magnetic Field Strength Matters
Effective brain stimulation requires sufficient magnetic field intensity. To meaningfully impact BDNF and brain recovery, the magnetic field must reach and engage deep neural tissues.
Research indicates that to achieve approximately 15 Gauss (G) at the target brain tissue—enough to influence inflammation and repair—a system needs to generate a surface intensity of around 4,000 G, due to the natural attenuation of magnetic fields through the skull (typically 15 cm thick). Daily sessions, over several weeks or months, may be required to see measurable benefits.
What cannot always be healed can often be maintained—and this is especially true for chronic neurological conditions.
Curious About PEMF for Brain Health?
At DrPawluk.com, we provide free consultations to help you choose the right PEMF system for your goals—whether you’re supporting recovery, addressing mood or cognitive challenges, or exploring proactive brain wellness.
Could magnetic field therapy become part of your care?
The evidence continues to build—and for many, it’s already making a meaningful difference.
Learn More
- Book a Free PEMF Consultation with one of our medical experts → https://www.drpawluk.com/
consult/ - Reference: Yalachkov Y., Karimi-Abdolrezaee S. et al., “Neuroplasticity in Multiple Sclerosis.” Frontiers in Neurology, 2025. (https://www.frontiersin.org/
journals/neurology/articles/ 10.3389/fneur.2025.1550152/ full) - For Safety Information about using PEMFs for the brain see: https://www.drpawluk.com/pemf-
safety/
Menopause and PEMFs
Menopause Transition Summit Interview with Dr. William Pawluk and Dr. Sharon Stills
tl;dr – Dr. Pawluk emphasizes PEMF therapy’s versatility and value as a foundational tool for health, particularly for women in menopause. Through regular use, PEMFs can address a wide range of menopausal symptoms, from sleep disturbances and hot flashes to bone density and cardiovascular health. This non-invasive, regenerative therapy represents a safe, effective way to enhance quality of life during the menopausal transition and beyond.
Overview
In an insightful interview between Dr. Sharon Stills and Dr. William Pawluk at the Mastering the Menopause Transition Summit, Dr. Pawluk, recognized as North America’s leading expert on Pulsed Electromagnetic Field (PEMF) therapy, discussed the profound benefits PEMFs offer for managing menopause symptoms and overall health. Dr. Pawluk, a holistic physician and former academic at Johns Hopkins, detailed his journey into PEMF therapy after witnessing the risks of conventional pain medications like Ibuprofen, which can cause life-threatening GI bleeds. Seeking non-invasive, safer alternatives, he initially studied acupuncture, then transitioned to using magnets for pain relief and healing. After observing rapid results, such as the accelerated healing of a spider bite, Dr. Pawluk’s interest in magnetic fields grew, leading him to co-author research and explore PEMF’s broader applications for health restoration.
PEMF Applications
PEMF therapy involves applying pulsed magnetic fields to the body, contrasting with static magnets, which rely on passive energy flow. Dr. Pawluk clarified that PEMFs work dynamically, pulsing magnetic energy into tissues and creating a “closed loop” field—safely directed and collapsing upon itself—unlike potentially harmful environmental EMFs. This dynamic nature allows PEMFs to permeate the entire body without damaging tissues, a fact Dr. Pawluk illustrated by comparing PEMF’s “wind-in-trees” effect: though unseen, it profoundly impacts cellular health and circulation. Importantly, Dr. Pawluk emphasized the need for high-intensity PEMF devices that deeply penetrate tissues to stimulate cellular repair effectively. PEMFs have been shown to increase cellular energy, promoting healing responses wherever the body needs it. This is particularly relevant for women facing menopause, who experience a broad range of symptoms from mood shifts to hot flashes, osteoporosis, and cardiovascular issues. According to Dr. Pawluk, PEMFs can mitigate these symptoms by helping the body regain its natural energy balance, or “charge,” vital for healing and functional regulation.
Cellular Regeneration
One of PEMF therapy’s major strengths is its role in cellular regeneration. Dr. Pawluk recounted a striking example of a young girl who regrew her fingertip using daily PEMF treatments after it was accidentally severed. This regenerative capacity is due to PEMFs’ ability to stimulate cell repair, ATP production, and stem cell activation. For women experiencing menopause, this means that PEMFs can help address tissue atrophy, improve skin elasticity, and stimulate collagen production, which naturally declines during menopause. In addition, Dr. Pawluk highlighted PEMF’s effectiveness in reducing inflammation, which is central to managing cardiovascular health—a leading concern for postmenopausal women. By targeting inflammation in blood vessels and the heart, PEMFs can reduce cardiovascular risks, including long-term effects of conditions like COVID-19, which has been associated with increased vascular inflammation.
Bone Health
PEMF therapy also supports bone health, a crucial factor for postmenopausal women who are prone to osteoporosis. Dr. Pawluk explained that while common medications like bisphosphonates slow bone loss, they don’t restore lost bone density, whereas PEMF therapy can actively stimulate bone formation. He stressed the importance of treating the entire skeletal system, not just typical DEXA scan sites like the spine and hips, as fractures in wrists, hands, and feet are also common. Regular, whole-body PEMF sessions can maintain bone density, enhance bone strength, and potentially reduce fracture risk. This preventive approach is valuable for those in early menopausal stages, as it provides a proactive defense against osteoporosis.
Symptom Management
For symptom management, PEMF therapy shows promise in relieving autonomic dysregulation, which underlies symptoms like hot flashes and insomnia. These symptoms are linked to imbalances in the sympathetic and parasympathetic nervous systems. Dr. Pawluk discussed how PEMF therapy could improve vagal tone, essential for reducing stress responses and supporting relaxation. He mentioned studies showing the benefits of high-intensity PEMF on the carotid artery, which can stimulate the vagus nerve. This stimulation helps modulate the autonomic nervous system, reducing hot flashes and improving sleep quality—a common concern among menopausal women. By enhancing sleep through increased melatonin production, PEMFs support deep, restorative sleep, an essential element for mood regulation and energy levels.
PEMFs and Cancer Levels
Dr. Pawluk also dispelled concerns about PEMF therapy exacerbating cancer, explaining that research largely indicates PEMFs do not promote cancer growth. Instead, PEMFs can be part of maintenance care for cancer survivors, helping strengthen bones and prevent osteoporosis—a frequent complication of cancer treatment. For women with breast cancer histories, PEMFs can help manage residual risks by maintaining bone health and reducing inflammation, supporting overall longevity and quality of life.
PEMF Recommendations
Regarding practical applications, Dr. Pawluk recommended whole-body PEMF devices to address systemic health and local PEMF devices for targeted relief. High-quality devices, such as those providing around 4,000 Gauss, are ideal, as lower-intensity devices often only provide surface-level benefits. He advised integrating PEMFs into daily routines for sustainable benefits, much like using a “magic mat” that one lies on each night to rejuvenate cellular energy. PEMFs work by creating a stable “charge” in cells, which slows aging processes, increases energy, and supports natural resilience. Additionally, Dr. Pawluk mentioned PEMFs as valuable adjuncts to bioidentical hormone replacement therapy (BIHRT), though he advised against depending solely on hormones, as PEMFs provide distinct anti-inflammatory and regenerative advantages.
Nutritional Supplement Tips
Because of our usual dietary habits and the quality of the food, as well as the normal stresses and demands of daily living, you never know on a day-to-day basis what essential nutrients you’re missing from your food. You often hear doctors say that supplements and vitamins only make for expensive urine. I say, better to have expensive urine than cheap urine! You absorb what you need and eliminate what you don’t. So, daily nutritional supplements and basic vitamins are necessary for almost everybody.
Supplement quality is directly related to supplement efficacy. The better the quality of your supplements, the better the job they will do for you.
To help ensure that you provide your body with sufficient amounts of the nutrients it needs to function at optimal levels, a good multivitamin/mineral is important. It will act as a security blanket, covering common diet deficiencies. In addition to a good multivitamin/mineral supplement, I recommend that most people take a basic foundation of nutritional supplements. These will support
the body’s general health regardless of underlying health conditions.
Basic foundation supplements I recommend to my patients include:
•Econugenics Pectasol powder, lime infusion – 2 scoops per day
•Purity’s Perfect Multi 2 twice a day or a similar quality multivitamin Vitamin D3 (2,000 – 5,000 IU daily)
•Omega-3 fatty acids (1,000 – 3,000 mg twice per day)
•Vitamin C (either a sustained-release formula of 1,000 mg twice per day, or general vitamin C 1,000 mg three times per day)—these are minimums.
•Magnesium (any form other than magnesium oxide) 350-500 mg/day
Curcumin, 500 mg twice a day to reduce inflammation (optional)
•Green tea extract, 500 mg twice a day for general well-being and prevention (optional)
When using PEMF therapies, maintaining proper levels of magnesium in the body is vital because PEMFs cause a great deal of calcium ion movement in the body. Magnesium is what calcium latches on to as it moves in and out of the cell, so a magnesium deficiency may undermine the effectiveness of PEMF treatments. Most good multivitamins, including the one recommended above, will provide adequate magnesium levels. Since most of us could use more magnesium, supplementation with it is recommended, especially when PEMF therapy is employed regularly.
We’ll be emailing regularly with tips and updates but, if you haven’t already, I would highly recommend reading my book : Supercharge Your Health With PEMF Therapy.
PEMFs and Parkinson’s (PD)
Table of Contents
PEMF treatment of Parkinson patient – Case Report
A 74-year-old retired building inspector with a 15-year history of Parkinson’s disease (PD) presented with a severe resting tremor in the right hand, generalized bradykinesia, difficulties with the initiation of gait with freezing, mental depression, and generalized cognitive impairment despite being fully medicated. Testing of constructional abilities employing various drawing tasks demonstrated drawing impairment compatible with severe left hemispheric dysfunction. He had two successive transcranial treatments, 20 minutes duration each, with pulsed electromagnetic fields (PEMFs) of very low intensity and frequencies of 5Hz and 7Hz. His tremor disappeared, and he had dramatically improved drawing performance. As he continued daily treatments with PEMFs for two more days, he had additional striking improvements in his drawing. This treatment demonstrates rapid reversal of drawing impairment in Parkinson’s disease, related to left hemispheric brain dysfunction even by brief transcranial very, low-intensity PEMFs. It also shows that cognitive deficits associated with Parkinsonism, which usually are progressive and unaffected by dopamine replacement therapy, may be partly reversed by these PEMFs. Treatment with PEMFs reflects a “cutting edge” approach to the management of cognitive impairment in Parkinsonism. (Sandyk, Sep 1997)
Parkinson’s Disease Introduction
Parkinson’s disease (PD) is the second most common neurodegenerative disorder in people over the age of sixty. Aging is the major contributing factor for increased risk of developing Parkinson’s disease. With the aging of the population worldwide, the frequency of Parkinson’s disease is expected to increase dramatically in the coming decades. Nearly one million people in the US are living with Parkinson’s disease. It is estimated that 6-10 million people worldwide have Parkinson’s disease, affecting all races and ethnicities. The incidence of Parkinson’s disease rises rapidly with age, affecting approximately 1% of the population older than sixty years and approximately 4% of those older than eighty years. Every nine minutes, someone in the United States is diagnosed with Parkinson’s disease. Parkinson’s disease (PD) is a chronic and progressive movement disorder primarily, meaning that symptoms continue and worsen over time. The cause is unknown, and there is no cure.
Conventional treatment options include medication and surgery to manage symptoms. Neither reduces progression.
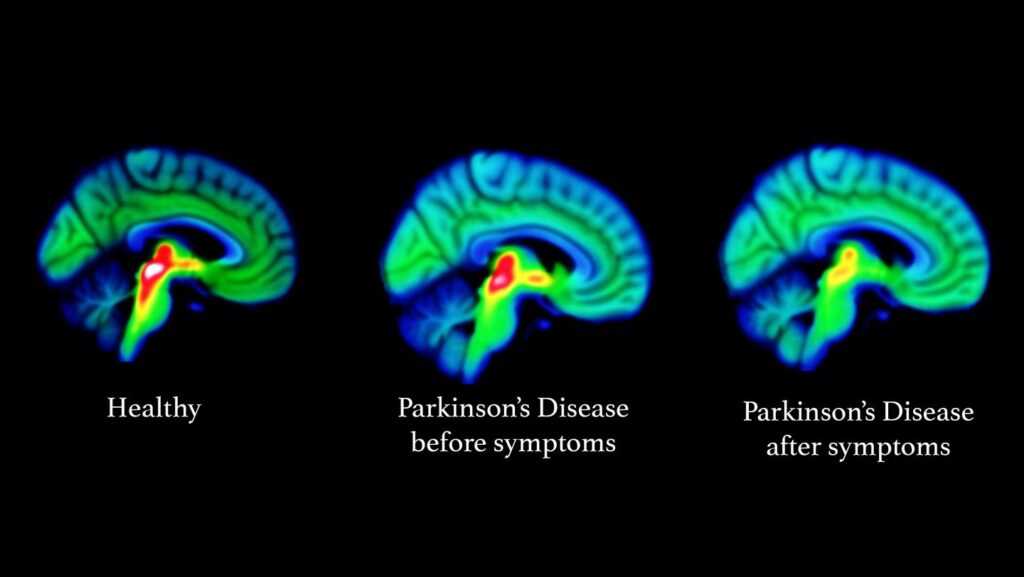
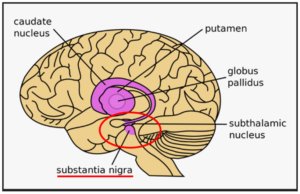
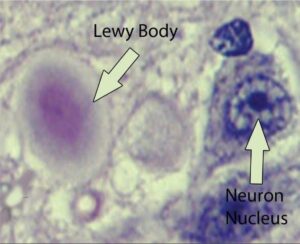 Parkinson’s disease most obviously involves the malfunction and death of vital nerve cells (neurons) in the brain, primarily an area of the brain called the substantia nigra. Some of these dying neurons produce dopamine, a neurochemical that sends messages to the part of the brain that controls movement and coordination. As Parkinson’s disease progresses, the amount of dopamine produced in the brain decreases, leaving a person unable to control movement normally. Loss of cells in other areas of the brain and body contribute to Parkinson’s. For example, researchers have discovered that the hallmark sign of Parkinson’s disease—clumps of a protein alpha-synuclein, which are also called Lewy Bodies—are found not only in the mid-brain but also in the brain stem and in scent cells. These areas of the brain correlate to non-motor functions such as sense of smell and sleep regulation. The presence of Lewy bodies in these areas could explain the non-motor symptoms experienced by some people with Parkinson’s disease before any movement (motor) signs of the disease appear. The intestines also have dopamine cells that degenerate in Parkinson’s, and this may be important in the gastrointestinal symptoms that are part of the disease.
Parkinson’s disease most obviously involves the malfunction and death of vital nerve cells (neurons) in the brain, primarily an area of the brain called the substantia nigra. Some of these dying neurons produce dopamine, a neurochemical that sends messages to the part of the brain that controls movement and coordination. As Parkinson’s disease progresses, the amount of dopamine produced in the brain decreases, leaving a person unable to control movement normally. Loss of cells in other areas of the brain and body contribute to Parkinson’s. For example, researchers have discovered that the hallmark sign of Parkinson’s disease—clumps of a protein alpha-synuclein, which are also called Lewy Bodies—are found not only in the mid-brain but also in the brain stem and in scent cells. These areas of the brain correlate to non-motor functions such as sense of smell and sleep regulation. The presence of Lewy bodies in these areas could explain the non-motor symptoms experienced by some people with Parkinson’s disease before any movement (motor) signs of the disease appear. The intestines also have dopamine cells that degenerate in Parkinson’s, and this may be important in the gastrointestinal symptoms that are part of the disease.
Standard medication treatment
Standard medication treatment of Parkinson’s disease can be only 50% effective overall. As the dose of taken medication is wearing off, there can be a decline in the drug’s efficacy. For example, in the morning shortly after taking it, the medication may be 90% effective, in the afternoon only 50% effective and in the evening only 30% effective. Twice-weekly treatments with extremely low intensity PEMFs applied to the head for ten weeks has been shown to eliminate these medication declining efficacy symptoms. At ten weeks after starting the PEMFs, there was 40% improvement in response to medication with minimum change in efficacy during the course of the day or evening. PEMFs appeared to enhance response to medication. Since decline in the response to medication is a phenomenon associated with progression of the disease, these results suggest that intermittent application of PEMFs may reverse the course of progressive Parkinson’s disease (Sandyk, Oct 1997).
Major aspects of Parkinson’s disease that are not addressed by conventional medical therapies, specifically pharmaceuticals, can be significantly impacted by PEMFs. These include: Neuro-inflammation, the Brain-Gut Axis, Ferroptosis, Mitochondrial Dysfunction, the Braak Hypothesis and Alpha-synuclein, Vagal Nerve Stimulation (VNS) and Deep Brain Stimulation (DBS), medication side effects, stem cell therapy, and comorbidities.
The major role of PEMFs in Parkinson’s disease is to impact multiple aspects of the condition, unlike most other therapies which tend to be one-dimensional. In any given individual with Parkinson’s disease there are often multiple factors that play into Parkinson’s disease, both in terms of initiation, progression and holistic management. PEMFs address multiple factors simultaneously because of their general actions in the body, covered in the books Power Tools for Health and Supercharge Your Health with PEMF Therapy and on the website DrPawluk.com. The impact of PEMFs on all of the above Parkinson’s disease contributing factors, are all covered in greater depth in the PEMFs and Parkinson’s Disease e-book. See the e-book section on Dr. Pawluk.com.
Pulsed Electromagnetic Fields (PEMFs) in Parkinson’s disease
The exploration of Pulsed Electromagnetic Fields (PEMFs) in Parkinson’s Disease (PD) represents an innovative frontier in neurodegenerative disorder treatment. The application of PEMFs offers a non-invasive method to potentially mitigate symptoms and alter the disease’s progression through mechanisms that influence cellular and neurological functions.
Electromagnetic stimulation of is a non-invasive rapidly emerging biological tissue treatment technique. PEMFs induce ion currents in the tissue and depolarize the electrical activity of all membranes, neurologic and non-neurologic slightly. Electromagnetic stimulation in animals and in the laboratory enhances cellular activity and stimulates growth-related responses and regeneration. As a result, PEMFs stimulate nerve growth and rebalance nerve abnormalities, increase microvascular blood flow and tissue oxygenation, and increase the amount and density of capillaries. As a result, PEMF treatment would be expected to delay disease progression and even induce neuro-repair in Parkinson’s disease. (Jensen)
Research on the use of PEMFs in Parkinson’s disease
| PD Symptom | Comments | Ref |
| Yawning and stretching | These are dopamine behaviors. Extremely low intensity PEMFs have been found to increase yawning and stretching. | Sandyk, Mar 1999 |
| Smell | The smell center of the brain also contains large amounts of dopamine neurons. Anti-Parkinson’s drugs do not affect the smell threshold. Low intensity PEMFs have improved smell in this situation. | Sandyk, Apr 1999 |
| Freezing, arrest of speech or handwriting | Difficulty in initiation and smooth processing of repetitive movements. Usually in PD of long duration and advanced stage and is a major cause of disability often resulting in falling. Seen as sudden attack of immobility usually experienced during walking, attempts to turn while walking, or while approaching a destination.
For resistance to medication, sometimes a reduction or increase in dose may improve this. Brief low intensity PEMFs improve freezing. The effect of each PEMF treatment lasted several days before appearing again. Weekly PEMFs to the head reduced freezing by ~ 50% and falling by ~ 80-90%, in a six-month follow-up period. |
Sandyk, 1996 |
| Disorder of body image | A part or parts of bodies perceived as disproportionately large. Low intensity PEMFs have reversed this. | Sandyk, Feb 1998 |
| Speech impairments | More than 89% of PDs. Speech impairments, including severe stuttering, that responded only marginally to medication, improved dramatically.
when PEMF treatments given weekly over four years. The speech impairment reappeared when regular PEMF treatments missed. |
Sandyk Nov 1997 |
| Cognitive impairment | Assessed by drawing tasks, eg drawing a picture of oneself, a bicycle, or a clock face. Drawing impairments indicative of dysfunction of half of the brain. PEMFs of 5 and 7 Hz for 20 minute periods dramatically improve drawing performance, even as soon as after 2 treatments. Drawing performance continues to improve as PEMF treatments continue. | Sandyk, SEPT 1997 |
Very Low intensity PEMFs
Dopamine is considered the most important part of the causes of Parkinson’s disease and is the primary target of medical therapies. Yawning and stretching are dopamine behaviors. When these behaviors are seen in people with neurodegenerative disorders, it is likely that they indicate release of dopamine in the brain. Extremely low intensity PEMFs have been found to increase yawning and stretching.
Various groups also looked at the use of low intensity 8 picoTesla PEMFs in the treatment of Parkinson’s disease, at 2 Hz or 8 Hz, for thirty minutes every forty-eight hours for sixty days. The treatment effects last beyond the time of stimulation depending on symptoms:
less than – 24 hrs for motor impairment,
- 48 hrs for activities of daily living, and
More than – 48 hrs for other symptoms
This shows that chronic stimulation is probably necessary to obtain adequate results with Parkinson’s disease (Bardasano).
The work by Sandyk, with the use of very low intensity PEMFs) also showed that longer-term treatments are necessary to achieve more sustainable results.
Medium intensity transcranial PEMFs
One study looked at a 25 Hz PEMF with intensity of 10 mT (100 gauss) applied for 20 minutes with 10-12 exposures as part of comprehensive rehab therapy in Parkinson’s disease patients. Walking improved significantly and so did the ability to change position. Muscle tension in the lower extremities was reduced in 85% of the patients, vertebral complaints in 85%, and general improvement was reportedly improved in 96% (Jerabek).
In another double-blind clinical study, 97 participants (Hoehn & Yahr stages I-IV) receiving optimal medical anti-Parkinson treatment, were randomized to either active or placebo treatment. Treatment was with transcranial PEMFs daily for a 30-minute home treatment for eight consecutive weeks. The PEMF was 5-8 mT using seven coils over the forehead, two on each side of the head and one in the back of the head. The Parkinson’s Disease Questionnaire (PDQ) was used at baseline and at the end. The active group improved in mobility and activities of daily living (ADL), compared to the placebo group. (Morberg, 2018)
The same group used the same PEMF and protocol on 92 study participants. (Morberg, 2017) Those receiving active treatment had an average age of 67, mean Hoehn & Yahr stage of 2.4, and disease duration of 6 years. In this study the Unified Parkinson’s Disease Rating Scale (UPDRS) was used. There were essentially no differences between the groups. The UPDRS scale is subjective and relatively insensitive and does not exclude the possibility of positive objective physiologic effects, compared to the PDQ.
High intensity PEMFs – repetitive Transcranial Magnetic Stimulation (rTMS)
High intensity PEMFs have been in use to stimulate the brain since 2008 after FDA approval. One type is called repetitive Transcranial Magnetic Stimulation (rTMS). In rTMS, a wire coil is used to generate a magnetic field that can pass through the scalp and the skull to change the excitability in the cortex according to the frequency. High-frequency rTMS (≥5 Hz) – a more rapid pulse rate (pulses per second pr PPS for short) ) induces more excitability in the cortex, while low-frequency/pulse rate rTMS (≤1 Hz) induces an inhibitory effect. A longer duration of stimulation is likely to induce a longer duration of effect. Additionally, there are numerous choices of stimulation sites of rTMS intervention; these sites include the primary motor cortex (M1), which is used mostly for motor symptoms; the dorsolateral prefrontal cortex (DLPFC) is used mostly for depression; the supplementary motor area (SMA) for motor symptoms; and, the cerebellum. The SMA is involved in a variety of cognitive and motor-related processes, in particular, the function of complex chains of movement. (Schramm). rTMS to the cerebellum showed an improvement in stroke (spasticity, balance, and gait), cervical dystonia, Parkinson’s disease (tremor), cerebellar ataxia, and essential tremor but not in multiple sclerosis. (Xia)
Astrocytes (start shaped cells) are specialized brain cells, outnumbering neurons by over five times. Astrocytes are also known collectively as astroglia, and are part of the glial cells in the brain and spinal cord. (Sofroniew) So, the terms astroglia and astrocytes are often used interchangeably. They “tile” the entire central nervous system (CNS) and exert many essential complex functions in the healthy CNS. Brain astrocytes respond to damage and disease in the central nervous system (CNS) through a complex, multifaceted process, called astrogliosis. Dysfunctions of astrocytes (astrogliosis) can lead to or contribute to a variety of CNS disorders. Astroglia/astrocytes undergo significant structural changes in response to CNS damage and disease.
Reactive astrogliosis and exaggerated pro-inflammatory reactions are key pathologic processes in Parkinson’s disease. rTMS has been shown to alleviate neuroinflammation. Higher frequency/pulse rate stimulation of rat brains daily for four weeks had a stronger anti-inflammatory and neuroprotective effect. The Endocannabinoid system (ECS) is integral to neural protection. PEMFs have been found to stimulate the ECS. Actions on the ECS by rTMS are a likely major mechanism of neural protection and anti-inflammatory action positively impacting reactive astrogliosis. (Aceves-Serrano)
High intensity PEMFs like rTMS improve the movement problems of Parkinson’s disease by about 54% overall. Results are better when high pulse rates greater than 5 pulses per second (pps) are used to the motor cortex, for 23% improvement. Results were better for lower than 1 pps applied to the front parts of the brain, with about 50% improvement. A greater number of pulses per session or across sessions have larger benefits. Given the limitations of rTMS treatments, that is, requiring a professional setting with a limited number of treatment options, it appears that treating for more than a week is not much better than treating for less than a week. But this appears to be driven by the number of pulses delivered (Chou).
One rTMS study looked at the treatment of 49 Parkinson’s disease patients. Their symptoms had been well controlled for three months with medications. Patients were divided into four groups to receive various protocols of rTMS with stimulation:
(1) once a day at 3,450 gauss;
(2) twice a day at 3,450 gauss;
(3) twice a day at 5,750 gauss;
(4) twice a day at 8,050 gauss.
Treatments took place for 10 days. The patients were evaluated 3 times before rTMS to obtain baseline data, then on days 3 and 7 of treatment, and then at 1 and 3 months after the end of treatment. They measured range of movement and disability in activities of daily living and short-term memory. In group 1, treatment once per day, there were no significant changes in symptoms at any time. By contrast, all other groups (receiving treatment twice per day) had significant improvement in symptoms at the 1-month assessment. But there were no differences in scores between the treated groups. At the 3-month evaluation point, the Parkinson’s disease symptom scores were still significantly better than baseline values but there were significant inter-group differences, with group 3 (twice a day at 5,750 gauss) showing the most improvement. The results show that this protocol causes long-lasting dose-related symptom improvements in Parkinson’s disease and may even allow dose reduction in medication (Mally).
In another rTMS study, Parkinson’s disease patients were evaluated to see if rTMS could improve muscle function assessed by simple reaction times. It had been previously shown that simple reaction time was significantly improved in normal individuals and in those with Parkinson’s disease. Assessments were done at the time of peak medication effect. For comparison, the same tasks were studied in ten normal volunteers. There were significant differences between Parkinson’s disease patients and normal volunteers during rTMS with the coil on the head. In Parkinson’s disease patients, rTMS significantly shortened reaction time and movement time without affecting errors. The mean performance of Parkinson’s disease patients improved during rTMS and patients reported that it was easier to perform the test during rTMS. All patients were significantly slower in the unmedicated state compared with the medicated state. Their performance in the unmedicated state improved significantly with PEMF stimulation (Pascual-Leone).
In a separate analysis of multiple studies, they evaluated the possible value of rTMS on cognitive function in Parkinson’s disease. They evaluated 12 studies and found that there was a mild short-term effect of rTMS on global cognition, executive function, attention and working memory. There were no significant benefits for long-term outcomes. The authors noted that more research is needed with larger numbers of individuals being tested. (He)
There is a frequently expressed concern about using high intensity PEMFs to the brain. Because some studies have suggested that an increase in stimulation pulse rate might enhance therapeutic efficacy, a randomized controlled trial was conducted (Benninger) using 50 pps/Hz rTMS in 26 individuals with mild to moderate Parkinson’s disease. Stimulation was to the motor cortex in 8 sessions over 2 weeks. Testing included evaluation of gait, slow movement, UPDRS and additional clinical, neurophysiological and neuropsychological elements. In addition, they studied the safety of our TMS with electromyography – electroencephalogram (EMG – EEG) monitoring during and after stimulation. The 50 pps rTMS did not improve gait, slow movement and global and motor UPDRS measures. There was a short-lived improvement in ADL. The neurophysiological and neuropsychological measures did not change. EMG/EEG showed no pathological increase of brain action or epileptic risk. There were no adverse effects. So, while this study did not find any clear benefits in movement and functional status, it did reveal the safety, even in those with Parkinson’s disease. Unfortunately, this research focused on stimulation of the motor cortex and not on the source lesions of the Parkinson’s disease in the substantia nigra/subthalamic nucleus. So, at this point it is not known whether stimulating the damaged tissue directly would produce any better benefits.
Parkinson’s disease has traditionally been considered a single-region disease in the basal ganglia but has recently been proposed as a system-level disorder that includes functional interactions between brain regions such as the dopamine dependent motor circuit (cortico-striatal-thalamic circuit) and the cognitive circuit (frontal-striatal circuit). However, structural changes in the brain take time to be produced and eight weeks of treatment is unlikely to be sufficient. Thus, even longer treatment periods are needed to better understand the potential of this treatment modality (Jensen)
Physiologically, it is known that erythropoietin (EPO), vascular endothelial growth factor (VEGF), as well as dopamine are present in the brain. EPO has neuroprotective benefits and neuro repair as seen in animal studies. In spinal cord traumatic injury and Alzheimer’s animal research, EPO improved memory and spatial learning and had a neuroprotective effect. VEGF affects growth of new blood vessels (angiogenesis), neural migration and neuroprotection and, along with EPO has the potential to help neurological disorders.
Since it was speculated that PEMFs could enhance neuroprotection, research was done to test this theory that long-term treatment with transcranial PEMF (T-PEMF) would improve motor performance (in terms of movement speed) and stimulate production of neuroprotective and angiogenetic compounds (EPO and VEGF) in the brain in patients with Parkinson’s disease. (Jensen) Using the same protocol as Morberg, the authors tested the idea that long-term treatment with T-PEMF would improve motor performance (in terms of movement speed) and stimulate production of neuroprotective and angiogenetic compounds (EPO and VEGF) in the brain in patients with Parkinson’s disease.
The active T-PEMF treatment group had 16 patients and 8 were included in the Parkinson’s disease-control no T-PEMF treatment group. Disease severity was assessed using the UPDRS. Daily 30 min home T-PEMF of 5-8 mT was applied for three eight-week periods, separated by one-week pauses. The total treatment period was 26 weeks. The primary outcome was movement speed, which was assessed in a timed six-cycle sit-to-stand (STS) task, where the participants were asked to perform the task as fast as possible. Examinations were done at week 17 and week 27. Eight patients from the T-PEMF group had lumbar puncture just before treatment and within one day after treatment completion for their brain EPO and VEGF levels. Results of the STS test improved progressively over the 26 weeks by about 20%. At the previously studied (Morberg, 2017) 8 wk study point it improved only by about 8%. The graph below (taken from Jensen), shows that 26 weeks of treatment improved STS (green line) from 100% at baseline (0%) to 80%. The control group (redline) got worse over that time by about 2%.
Spinal fluid (CSF) EPO concentrations increased significantly in response to the T-PEMF treatment intervention (all patients increased (n = 8)). CSF-VEGF concentration increased in five out of six patients. So, it appears that T-PEMF treatment has contributed to neural repair and protection of the dopamine neurons in this study. In addition, importantly, there was no difference between the longer treatment time group and the placebo group regarding reported adverse events.
The previous study (Morberg, 2017) showed that an eight-week treatment period was beneficial for patients with mild Parkinson’s disease whereas the treatment effect was less among the more severely affected participants. However, the present study (Jensen) treatment for 30 min/day for 3×8 weeks showed a benefit for the entire study group including mild as well as more severely affected Parkinson’s disease patients. It’s also plausible that the longer treatment time would have impacted the amount of EPO and VEGF more as well. Finally, even though the treatment group was well medicated, T-PEMF treatment still improved the completion time in the STS-task by 19%, comparably to the healthy control group. This shows that the PEMF treatment improves significantly on the benefits seen from medication management. The question then becomes whether medication management is necessary when doing more intensive longer-term PEMF therapy. However, this difference in benefit may only apply to this study and to the motor function studied, and may not apply to the other aspects of dysfunction in Parkinson’s disease.
Freezing of Gait (FOG): The effect of rTMS has been studied on FOG. However, stimulation of neither the motor cortex nor the frontal cortex showed benefit in one study. (Kim KW). Another stimulation site, The supplementary motor area (SMA) has also been explored. When tested on 30 Parkinson’s disease patients with FOG, it was shown that 10 sessions of 10 pps rTMS over the SMA improved FOG (Mi). This study also found that the benefit could last at least 4 weeks after stimulation. This result was consistent with those of another study (Kim SJ), where they found significant improvements after 2 sessions of high-PPS SMA stimulation in 12 Parkinson’s disease patients, but not after motor cortex stimulation. These results suggested that SMA stimulation may be a more appropriate target in Parkinson’s disease patients with FOG.
How to use PEMFs for the treatment of Parkinson’s disease
PEMFs can be extraordinary helpful in the care of Parkinson’s disease and are even more valuable considering that no other therapies to date have been able to cure it or stop its progression. Even the standard medication, the primary line of treatment for Parkinson’s disease, is only about 50% effective overall to help with the symptoms of Parkinson’s disease. While research is ongoing to develop new therapies and approaches, PEMF therapy has a long history of helping a myriad of different health conditions, safely and without risk. In fact, when somebody owns a PEMF device, not only do they benefit across many different health needs, but it can also be used by other family or household members, including pets. There are many scientifically backed examples of the extent of usefulness of PEMFs in the book “Power Tools for Health” (Pawluk), including a section on its use for Parkinson’s disease.
As mentioned earlier, even twice-weekly treatments twice-weekly treatments with extremely low intensity PEMFs applied to the head for ten weeks has been shown to eliminate the daily drop-off of medication benefit. (Sandyk, Oct 1997) At ten weeks after starting the PEMFs, there was 40% improvement in response to medication with minimum change in efficacy during the course of the day or evening. They have even been found to be helpful for the side effects of the medications. In addition, since decline in the response to medication over time in patients with Parkinson’s disease is associated with progression of the disease, even intermittent application of PEMFs may reverse the course of progressive Parkinson’s disease.
Those results are based on a health services delivery model requiring that the treatment be provided in a doctor’s office. This is not only inconvenient and also expensive over time, but also increases the risk of progressive disease. As Parkinson’s disease progresses, becomes much more difficult to manage, and as a result there is a much greater toll on the health, function and vitality of the person.
Overall health
Because of all the different actions of PEMFs, reviewed in “Power Tools for Health“, PEMFs are not just a treatment for Parkinson’s disease but also overall health. Any other health demands place a significant strain on the body in coping with Parkinson’s disease, and increase the risk of more rapid progression. As a result, PEMFs not only help with Parkinson’s disease but any other health conditions (comorbidities) as well. Since Parkinson’s disease typically begins after age 50, and especially after age 60, comorbid conditions are common. Per the CDC many people have have 2 or more comorbid conditions: 33% of those between 45-64 years of age and 64% of those 65 or older. (Boersma)
Progression of PEMF benefits
As PEMFs are used there is a progression of benefits, dependent on the amount of healing that happens with use. Often there are significant improvements in symptoms in the first few days to weeks. The extent of these improvements may depend on the pace of increasing treatment time and intensity, that is, the “going low and slow” progression. Clearly, the lower the intensities used and the less the treatment time, the less the expected benefit. While anybody can get benefit even at the lower intensities and time, the better benefits will happen with more treatment time and higher magnetic field intensities.
After the initial “blush” of changes in symptoms, with continuing treatment there will be gradual improvements in function, either improved function over normal or less functional disability. As healing continues, the improvements in symptoms and function last longer and are less likely to return as quickly. There may come a time when there appear to be no further improvements in symptoms and function. People often worry that this means that “tolerance” to the magnetic field therapy is happening. This just means that the “low hanging fruit” of the benefits of PEMFs have been achieved. At this point continued therapy will be working at the deeper levels of healing, at the cellular level. Cellular level healing tends to take longer, especially with the brain, and is much less obvious and noticeable. I can generally say that “cells don’t talk to you” but tissues and organs do. When enough of the deeper cellular healing accumulates, the improvements become more noticeable and are less likely to regress when treatment is reduced. If treatment is reduced too soon, symptoms are more likely to recur. Generally, the longer it takes symptoms to recur after stopping or reducing treatment, the deeper the healing. But if symptoms do recur that means that healing is not completed. It’s possible that some levels of damage in the body can never be completely fixed and we may have to accept the level of gain obtained to that point.
Let’s not forget that Parkinson’s disease is not just a brain disorder. It is a systemic disorder that has brain effects as a major manifestation. Most of the things that happen to the brain and nervous system from the PEMFs are also happening in the rest of the body. In Parkinson’s disease jargon, there are the motor benefits and the nonmotor benefits. PEMFs help with both groups of needs. The order in which they are helped is controlled by the body and we can prioritize which ones are going to be helped first, and so forth.
In the treatment of Parkinson’s disease, the actions of PEMFs that are most important (Pawluk) include reductions in:
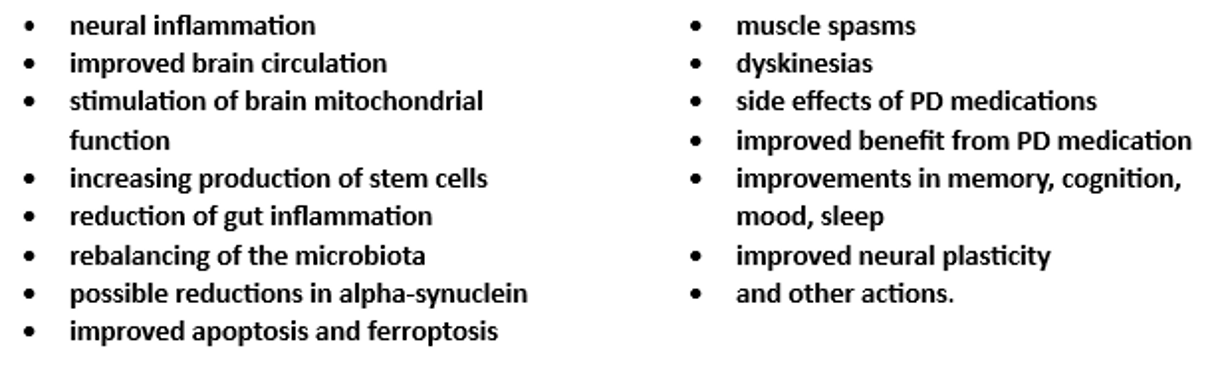
Magnetic field intensity matters
The intensity of the magnetic field is very important in being able to reach deep into the brain with sufficient magnetic field intensity to reduce inflammation and stimulate many of the other actons of PEMFs. Our experience is that the benefits of very low intensity PEMFs that have been published are typically not long-lasting and not as beneficial as higher intensity PEMFs, as can be seen from the research on rTMS. The challenge in showing long-term effectiveness of rTMS is because of the nature of rTMS research. It usually has not been done long enough to see sustainable and significant benefits.
It is recommended to read about the role of adenosine in reducing inflammation in the body and that the optimal magnetic field intensity for the best impact on inflammation. More can be read about this at https://www.drpawluk.com/pain-inflammation-adenosine/. Also, it is strongly recommended to read the books https://www.drpawluk.com/product/power-tools-for-health/ and https://www.drpawluk.com/product/supercharge-your-health-with-pemf-therapy/ for more in-depth information on PEMF therapies. The “Power Tools for Health” book has over 500 references for those who wish more of the scientific background. The “Supercharge Your Health” gives much more practical advice on the use of PEMFs, in general and more specifically for about 80 different health conditions.
Further advice
Given the progression of Parkinson’s disease over time and the irreversibility of the physical changes with later stages of Parkinson’s disease, it is strongly recommended to start as early as possible, certainly at the time of initial diagnosis. As screening tests become more available it may be possible to start treatment for prevention purposes very early, before motor symptoms become obvious. Tests are becoming available now for detecting early levels of alpha-synuclein either with intestinal biopsies or spinal fluid. Inflammation is a major driver of causing aggregation of the normal tissue levels of synuclein. As the research is showing, once the aggregated synuclein begins, it starts to migrate, eventually ending up in the nervous system. One of the key drivers of the aggregation of synuclein is inflammation, whether in the gut or elsewhere in the body. Therefore, starting as early as possible in the course of the disease is essential to limit its progression and limits the course of the disease.
Because of its chronic local and systemic nature, lifetime daily home use of a PEMF system with adequate intensity is recommended before irreversible damage happens in the body, and especially in the brain. The minimum recommended intensity is about 4000 Gauss, to be able to reach deep into the abdomen and across the brain. Treatment to the brain should be at the top of the neck with the applicators placed from the back of the head toward the front of the brain. Additional placements could be of a double loop coils over the top of the head, with a loop over each ear. If there are significant cognitive, memory and mood issues, placements could also be across the front of the head. Ultimately, each individual will have to use trial and error to determine the best placements.
In addition to local treatments to the brain, daily or even twice daily whole-body treatment should also be used.
PEMF therapies can be combined readily with almost any other kinds of therapies, and should usually include neuro-supportive nutrition and supplements. PEMFs can also be combined with almost any other kinds of complementary therapies, although many of these do not work deep enough. These other therapies can include red light, intravenous nutrients, such as IV vitamin C, glutathione, and alpha lipoic acid (ALA). It is advised to seek the support of a clinician/professional who is familiar with recommending supplements for neurological disorders. Some of this information about combining PEMFs with other therapies is found in the two books mentioned above.
Resources
https://www.drpawluk.com
https://www.drpawluk.com/pain-inflammation-adenosine/.
https://www.drpawluk.com/product/power-tools-for-health/ https://www.drpawluk.com/product/supercharge-your-health-with-pemf-therapy/
PEMF consultations
To be certain to obtain the right PEMF system and be trained in its proper use, it is recommended to seek the support of a licensed professional who is familiar with PEMF therapy and other complementary therapies to go with it. It PEMF therapies are recommended, always ask about the intensity of the PEMF system being used. Remember, that office-based treatments are not going to be done affordably over extended periods of time to be certain that the best results will be obtained, especially considering that treatment should be lifetime. As yet, there is no cure still, even with PEMF therapy, so, basically, lifetime maintenance and control is necessary as far as we know.
Consultations without charge are available on Dr. Pawluk.com. https://www.drpawluk.com/consult/
Summary
So, it appears that PEMFs of various intensities and treatment times can be helpful in the management of Parkinson’s disease. Longer treatment times and stronger PEMFs are very much likely to produce better and more lasting results. Since the goal is to help to repair the brain, not just improve function temporarily, long-term treatment frequently appears to be necessary. What is not known is whether the combination of periodic high intensity PEMFs along with a home therapy program using a lower intensity PEMF system may be the most helpful. It also appears that PEMFs may be synergistic with medication, which has a history of losing its effectiveness over time. It is not known how well PEMFs alone, without medication, may be able to help the symptoms and progression of Parkinson’s disease. At this point at least, there’s still no clear evidence that PEMFs can “cure” the condition. Much of the research with rTMS follows typical protocols, either to the motor area of the brain or the left frontal lobe. I have not seen any research that focuses treatment directly over the anatomic area in the brain, that is, the substantia nigra, primarily involved in the condition. Whole body treatment is recommended, in addition to the brain, because it appears that the origins of Parkinson’s disease may well be elsewhere in the body, especially in the intestinal tract.
References
- Aceves-Serrano L, Neva JL, Doudet DJ. Insight Into the Effects of Clinical Repetitive Transcranial Magnetic Stimulation on the Brain From Positron Emission Tomography and Magnetic Resonance Imaging Studies: A Narrative Review. Front Neurosci. 2022 Feb 21;16:787403.
- Benninger DH, Iseki K, Kranick S, et al. Controlled study of 50-Hz repetitive transcranial magnetic stimulation for the treatment of Parkinson disease. Neurorehabil Neural Repair. 2012 Nov-Dec;26(9):1096-105.
- Boersma P, Black LI, Ward BW. Prevalence of Multiple Chronic Conditions Among US Adults, 2018. Prev Chronic Dis 2020;17:200130.
- Chou YH, Hickey PT, Sundman M, et al. Effects of repetitive transcranial magnetic stimulation on motor symptoms in Parkinson disease: a systematic review and meta-analysis. JAMA Neurol. 2015 Apr;72(4):432-40.
- He PK, Wang LM, Chen JN, et al. Repetitive transcranial magnetic stimulation (rTMS) fails to improve cognition in patients with Parkinson’s disease: a Meta-analysis of randomized controlled trials. Int J Neurosci. 2022 Mar;132(3):269-282.
- Jensen BR, Malling ASB, Schmidt SI, et al. (2021) Long term treatment with transcranial pulsed electromagnetic fields improves movement speed and elevates cerebrospinal erythropoietin in Parkinson’s disease. PLoS ONE 16(4): e0248800.
- Jerabek, J and Pawluk, W. Magnetic therapy in Eastern Europe: a review of 30 years of research. Publ. Advanced Magnetic Research of the Delaware Valley, Chicago, 1996.
- Kim SJ, Paeng SH, Kang SY. Stimulation in supplementary motor area versus motor cortex for freezing of gait in Parkinson’s disease. J Clin Neurol. 2018;14(3):320–326.
- Kim YW, Shin IS, Moon HI, Lee SC, Yoon SY. Effects of non-invasive brain stimulation on freezing of gait in Parkinsonism: a systematic review with meta-analysis. Parkinsonism Relat Disord. 2019;64:82–89.
- Mally J and Stone TW. Therapeutic and “dose-dependent” effect of repetitive microelectroshock-induced by transcranial magnetic stimulation in Parkinson’s Disease. J Neurosci Res 57(6):935-940, 1999.
- Morberg BM, Malling AS, Jensen BR, et al. Parkinson’s disease and transcranial pulsed electromagnetic fields: A randomized clinical trial. Mov Disord. 2017 Apr;32(4):625-626.
- Morberg BM, Malling AS, Jensen BR, et al. The Effects of Transcranial Pulsed Electromagnetic Field stimulation on quality of life in Parkinson’s Disease. Eur J Neurol. 2018 Mar 23.
- Pascual-Leone A, Valls-Sole J, Brasil-Neto JP, et al. Akinesia in Parkinson’s disease. ii. Effects of subthreshold repetitive transcranial motor cortex stimulation. Neurology 44(5):892-898, 1994.
- Pawluk W and Layne CJ. Power Tools for Health: how magnetic fields (PEMFs) help you. Publ. Friesen Press, 2017.
- Sandyk R. Freezing of gait in Parkinson’s disease is improved by treatment with weak electromagnetic fields. Int J Neurosci. Mar;85(1-2):111-24, 1996.
- Sandyk R. Reversal of a body image disorder (macrosomatognosia) in Parkinson’s disease by treatment with AC pulsed electromagnetic fields. Int J Neurosci. Feb;93(1-2):43-54, 1998.
- Sandyk R. Reversal of cognitive impairment in an elderly parkinsonian patient by transcranial application of picotesla electromagnetic fields. Int J Neurosci. 1997 Sep;91(1-2):57-68.
- Sandyk R. Speech impairment in Parkinson’s disease is improved by transcranial application of electromagnetic fields. Int J Neurosci. Nov;92(1-2):63-72, 1997.
- Sandyk R. Treatment with AC pulsed electromagnetic fields improves olfactory function in Parkinson’s disease. Int J Neurosci. Apr;97(3-4):225-33, 1999.
- Sandyk R. Treatment with AC pulsed electromagnetic fields improves the response to levodopa in Parkinson’s disease. Int J Neurosci. Oct;91(3-4):189-97, 1997.
- Sandyk R. Yawning and stretching induced by transcranial application of AC pulsed electromagnetic fields in Parkinson’s disease. Int J Neurosci. Mar;97(1-2):139-45, 1999.
- Schramm, S., Albers, L., Ille, S. et al. Navigated transcranial magnetic stimulation of the supplementary motor cortex disrupts fine motor skills in healthy adults. Sci Rep 9, 17744 (2019).
- Sofroniew MV. Astrogliosis. Cold Spring Harb Perspect Biol. 2014 Nov 7;7(2):a020420.
- Xia Y, Wang M, Zhu Y. The Effect of Cerebellar rTMS on Modulating Motor Dysfunction in Neurological Disorders: a Systematic Review. Cerebellum. 2023 Oct;22(5):954-972. Parkinson’s disease
PEMF MACHINES RISK AND POTENTIAL DANGERS OF PEMF THERAPY
The only absolute contraindication for use of a PEMF device is placing an active applicator over implanted electrical devices like pacemakers, cochlear implants, intrathecal pumps, etc., because the magnetic field can shut the device off or otherwise interfere with its function.
PEMFs are contraindicated in organ transplant patients. This is because these people are on immune suppression medications to prevent organ rejection. We do not want to risk adversely affecting the immune suppression/rejection process. There is a chance that PEMFs may actually stimulate or activate a more aggressive rejection process by stimulating the immune system.
USING YOUR PEMF MACHINE SAFELY
Safety of PEMFs has not been established in pregnancy, although there is no evidence of harm. Most manufacturers warn against the use of their device during pregnancy.
PEMFs should be used with caution in Grave’s disease or in the case of active bleeding.
Extremely high intensity PEMFs (> 5000 Gauss) should be used with caution or with professional guidance in people with implanted metals, such as joint replacements, dental implants, mechanical heart valves, metal stents, or metal staples in blood vessels. This is not due to risk of injury or harm, but because these PEMFs may stimulate the nerves in the area of the metal, causing sharp pain. With any of these situations “going low and slow” https://www.drpawluk.com/going-low-and-slow/ is recommended to determine optimal intensity level. These PEMFs may also add to the shear stress of metal clips placed in or near blood vessels.
High intensity PEMFs over breast implants used to be considered a possible risk to the implant material. Women are now being recommended to do breast MRIs periodically due to the inflammation-related breast health risk. If there is considered to be no risk from MRI, PEMFs would be expected to be safe. Use of high-frequency PEMFs beyond 1000 Hz are probably also not desirable for treatment durations longer than an hour at a time, given the risk of agitating the plastic or silicone in breast implants, resulting in possible thinning and risk of leakage.
SELECTING A PEMF SYSTEM – THE FIRST ESSENTIAL STEPS
If you are considering getting a PEMF system for your health, the number of choices can be overwhelming. So, what are some of the most important considerations to make the right choice?
Since getting a PEMF system is an investment in your present and future health, it’s important to consider not only what is motivating you or other household members now but also having some idea of what you may need in the future. In this situation, because a PEMF system is an investment that will be available to you for years to come, it may be worth thinking about getting something better than you would consider just for the short term.
WHOLE BODY SYSTEM OR LOCAL PEMF SYSTEM?
The first decision needs to be whether you need a ‘whole-body’ PEMF system or a ‘local’ PEMF system.

Whole Body PEMF System

Local/Small area PEMF system
A local system will have applicators that are basically only useful to treat one small area of the body at a time, such as a hand, knee, elbow, foot, part of the shoulder, part of the back, prostate, bladder, or neck, etc.
A long and wide pad applicator will typically treat the entire body. Whole-body PEMF systems are typically used for health maintenance, since the whole body needs health maintenance. If you want to treat several local areas of the body at the same time, this can be done more easily, saving time, by using a whole-body system. Systemic health conditions such as osteoporosis, Lyme disease, Chronic fatigue syndrome, autoimmune diseases, vascular diseases, or multi-area skin disorders may normally also require a whole-body PEMF system.

Local PEMF System

Whole Body PEMF System
All whole body PEMF systems have smaller pad-type regional applicators that can be used separately from the whole-body pad. A regional applicator is one that treats an area of the body, for example, the abdomen, the chest, the pelvis, hips, shoulders, or upper or lower back. These are often also called pillow applicators and come in various sizes depending on the system. Whole body pads are almost always lower intensity than local or regional applicators/pads. So, you will need to know the intensity of each applicator.
WHAT MAGNETIC FIELD INTENSITY DO I NEED?
After deciding on local versus whole body, the next most important decision will usually be what magnetic field intensity is needed. My video “intensity matters” describes why magnetic field intensity is important. There are several choices among whole body PEMF systems ranging in intensity from 500 gauss to < 1 Gauss (< 100 micro Tesla). The rule of thumb is that the higher the intensity the faster the results and the less the treatment time.
Many people make their decision based on cost, sacrificing results. Results are often promised with very low intensity systems that ignore the research studies showing that higher intensity is needed. Many of these proven intensities can be found in Dr Pawluk’s book Power Tools for Health.
Health maintenance, done daily, may be reasonably effective with very low intensity systems or higher intensity systems. When someone wants to do health maintenance and there are significant health problems in multiple areas of the body, higher intensity whole body pads will be needed. These should preferably be over 50 Gauss (5000 microTesla or 5 milliTesla).
If you decided you needed a local treatment PEMF, the next most important consideration is intensity. Lower intensities may work well for superficial problems in tissues that are not deep in the body, such as the hands, elbow, shoulder tendinitis, carpal tunnel, heel spurs, eyes, teeth, TMJ, etc. Higher intensity local PEMFs are needed for problems deeper in the body, such as in the brain, spine, prostate, bladder, hips, knees, heart, lung, gallbladder, pancreas, kidneys, bones, etc. Local treatment PEMFs can range in maximum intensity from 10 Gauss to around 10000 Gauss.
If you want to do whole body and regional treatments with the same PEMF system, intensity also becomes very important. Regional applicators can range in intensity from <1 Gauss to 1500 Gauss.
Generally, the higher the intensity, the more expensive the PEMF.
Once the basic decision is made on whole body versus local, and the intensity needed, other considerations also come into play, including frequencies, applicator shapes, whether portable or AC powered, and whether rentals are available. Advice about the variety of PEMF options may be needed from someone knowledgeable to help sort out all the options.
Hopefully, this will help you to sort out some of the confusing information about which PEMF system is the best for you. For more information read my book Power Tools for Health or go to my website DrPawluk.com. There you can find more useful information on pulsed electromagnetic field treatment, such as PEMF intensities, frequencies & waveforms, how to apply PEMF, etc. We also offer a variety on whole-body PEMF systems and local PEMF systems.
Healing with PEMF Therapy

SETTING A HEALING TIMELINE FOR PEMF TREATMENT
One of the most common questions people have before starting PEMF therapy is about how quickly they will see results. The answer is dependent on a variety of factors and is impossible to predict with any great precision. That being said, we can usually help people manage their expectations and make an estimate as to when they may be able to expect some improvement by setting a healing timeline.
Determining when a person will feel better begins with understanding how PEMF therapy works when applied to various health conditions, and understanding the overall health of the person being treated. Device selection is exceptionally important to achieving the best, fastest, most sustainable results from your system.
Many people experience tremendous results within the first week or two of using their system. For some people, results come more slowly, and we can react to that by fine-tuning the treatment protocol. The body takes time to heal once it is given the appropriate signal or stimulus. A fracture, for example, will take 8 to 12 weeks to heal to a point where the bone can be used. This does not mean the healing process is complete, but just that the body part is usable once again. Magnetic therapies can speed the healing rate, but they cannot work miracles. Illness is rarely, if ever, an instantaneous happening—the same is true of healing. We did not get to our current health state overnight, and we are unlikely to heal overnight.
IMPROVEMENT AND HEALING WITH PEMF THERAPY
Setting a healing timeline and having proper expectations is important in the use of PEMF therapies. If you are depressed or anxious, for example, small health improvements may seem inadequate. To set realistic expectations, we must first understand the nature of the problem, the depth of the damage or dysfunction, the types of tissues involved and their respective regeneration potential, and the age of the person. In many cases, people don’t necessarily notice a huge improvement in symptoms day to day, but when they look back over a week or a month, they realize they have improved significantly.
Even if PEMFs are not likely to reverse a dysfunction, they can stall or slow the progression of a disease state. And for tissues that do not have regenerative capacities, PEMFs are still valuable in reducing pain, reducing swelling, improving circulation, and stimulating whatever regeneration may be possible.
Since many health problems for which PEMFs are being used are stubborn and chronic, it may take up to 6 months to achieve desirable results. If the treatment program is too gentle, or there is an inadequate amount of time spent on the system, results may not be seen in the first few months.
WHAT CAN PEMF THERAPY TREAT?
While the ways in which the body heals itself are known, there are various places in the healing process where the body may get “stuck”. This is where tissues are most vulnerable to the disease state progressing from acute to chronic. Cellular communication begins with a signal impulse and ends with a change in cellular behavior. When the cellular change is a destructive one, a condition can become chronic. Reestablishing normal cellular communication is the only way to combat the dysfunction.
Pain and inflammation are two of the most common conditions treated with PEMF therapies. Both can be categorized as either acute or chronic. Acute pain and inflammation in an otherwise reasonably healthy body will likely take care of themselves, though PEMF therapies are expected to streamline the process and speed up healing time. The earlier in the process you use PEMF therapies, the faster you will see results.
There are some health problems that cannot be corrected with PEMF therapy alone. One common example is with bone-on-bone arthritis in the knee or hip. In this circumstance, the damage is so extensive and so many tissues are involved that a joint replacement is often inevitable. Even in this situation, however, PEMF therapies can make a huge difference one way or another. If the magnetic therapy is not controlling the pain of the condition, it can assist the tissues to be as healthy as possible prior to having the joint replacement. After the surgery, the recovery time is expected to be shorter with the help of magnetic field therapy, and with a decreased risk of complications. In addition, some research and feedback from patients indicates that the prosthesis integrates better with the bone, making the new joint feel stronger. This osteointegration may also decrease the likelihood for future breakdown.
SENSITIVITY TO PEMF AND OTHER MAGNETIC FIELDS
Infrequently, we experience individuals who are extraordinarily sensitive to magnetic fields, and experience increased discomfort or other unpleasant symptoms. In these cases, PEMF therapy must be used “low and slow,” meaning with a low intensity, and short treatment times. In these cases, setting a healing timeline helps understand that benefits may be more difficult to achieve due to the appropriate and necessary intensities not being possible. Still, results can be dramatic. Most of these individuals need to be on a significant supplement and nutrition program to achieve the best results.
Research in the pain management program at Hopkins found that some individuals with chronic pain have personality traits that result in very poor treatment outcomes. These individuals often experience negative reactions even to placebo magnetic fields. When these patients are followed over time, some complain that their problems have been made worse by the (placebo) treatments. In these situations, it is not possible to please, and therefore PEMF therapy is not an appropriate treatment modality.
PEMFS AND BRAIN RECOVERY AFTER STROKE
Table of Contents
The ability to recover after stroke depends on many factors, including the regenerative capabilities of the brain. Recovery depends on the plasticity of the brain. The plasticity, or neuroplasticity, required in a damaged brain is very different from the plasticity of a normal functioning brain. The demand for adaptive healing starts immediately after a stroke event where blood supply to the brain is stopped or limited. The availability of various factors in the brain, called neurotrophic or growth factors, affect the potential for the growth of new neurons and the survival of existing neurons. Neurogenesis is regulated by many factors including neurotrophins, growth factors, hormones, neurotransmitters, and micro-environmental factors.
A PEMF STUDY IS CONDUCTED
A study was done to evaluate the effect of extremely low-frequency electromagnetic field therapy (PEMF) on brain plasticity in the rehabilitation of patients after stroke. (2)
The cerebral ischemic event (stroke) in each patient was documented by computer tomography (CT) scan of the brain. Neurological and CT findings were interpreted by 2 or more independent experienced neurologists. All patients were diagnosed with ischemic stroke. Patients with other types of stroke were excluded, as were patients with neurological illness other than stroke; chronic or significant acute inflammatory factors; and/or dementia.
Forty-eight patients were divided into two groups and had the same rehabilitation program. In both the groups, the program was provided by a physiotherapist, every day for a period of 4 weeks with weekend breaks. The rehabilitation program included 15 min of psychotherapy, 60 min neurophysiological session in the morning (30 min of function enhancing techniques and 30 min of repetitive task practice or balance) and 30 min aerobic training (2–3 times a day for 10 min at 60 min intervals).
Neurophysiological rehabilitation consisted mainly of functional rehabilitation techniques and repetitive task practice designed to intensively use the affected upper and lower limbs. The function techniques included activities based on activities of daily living (ADL). However, training time was individually modified depending on the improvement in motor function of the affected limbs, if necessary.
The rehabilitation program in the control group consisted of a 60 min session in the morning (30 min of function improvement techniques and 30 min of balance training), 30 min aerobic training (2–3 times a day for 10 min at 60 min intervals) and 30 min muscle strengthening exercises. The range of physical effort during the rehabilitation programs in both groups of patients was between 13 and 14 according to the Borg functional scale (moderate effort).
Most of the people in the study were between 3 to 4 weeks after their stroke and were on average between 45-48 years of age. In the pulsed electromagnetic field therapy (PEMF) study group, the patients additionally were exposed to a standard series of 10 PEMF treatments, for 15 mins each, at 5 mT (50 G), 40 Hz, to the pelvic girdle. The non-PEMF group received the same rehabilitation program, without PEMF therapy.
That’s right! PEMF treatment was to the pelvis, not to the brain, as would normally be expected. At the time of this research there was a concern about PEMFs precipitating seizures. This concern has largely been discounted with the FDA approved high intensity transcranial magnetic stimulation devices for treatment resistant depression, with seizures being extraordinarily rare and much less likely to happen with the relatively low magnetic field intensities used in this research. As it turns out, from this research, stimulation of the pelvic area with this PEMF set-up still ended up producing significant changes in levels of various biochemical markers. These biochemical factors end up in the circulation, and finally in the brain. In the brain they create various reactions that can help improve the negative effects of stroke.
This research group looked at many factors associated with the outcomes of stroke and associated these outcomes with treatment results. After 4 weeks, during which patients had undergone neurorehabilitation and neurological examinations, they assessed functional recovery using the Barthel Index, Mini-Mental State Examination (MMSE), Geriatric Depression Scale (GDS), National Institutes of Health Stroke Scale (NIHSS), and the modified Rankin Scale (mRS).
The modified Rankin Scale (mRS) is commonly used for measuring the degree of disability or dependence in the daily activities of people who have suffered a stroke or other causes of neurological disability. It has become the most widely used clinical outcome measure for stroke clinical trials.
RESULTS OF PEMF STUDY ON BRAIN RECOVERY AFTER STROKE
Any kind of damage to the brain causes the brain to adaptively respond. This adaptation process is called neuroplasticity. Neuroplasticity, also known as neural plasticity or brain plasticity, is a process that involves adaptive structural and functional changes to the brain. A good definition is “the ability of the nervous system to change its activity in response to intrinsic or extrinsic stimuli by reorganizing its structure, functions, or connections.” Clinically, it is the process of brain changes after injury, such as a stroke or traumatic brain injury (TBI).These changes can either be beneficial (restoration of function after injury), neutral (no change), or negative (can have pathological consequences). (2)
Neuroplasticity
Neuroplasticity can be broken down into two major mechanisms:
Neuronal regeneration/collateral sprouting: This includes concepts such as synaptic plasticity and neurogenesis.
Functional reorganization: This includes concepts such as equipotentiality, vicariation, and diaschisis. Vicariation is considered a mechanism for recovery of function following brain damage. Essentially, this concept involves the ability of one part of the brain to substitute for the function of another. Diaschisis is a sudden change of function in a portion of the brain connected to a distant, but damaged, brain area. The site of the originally damaged area and of the diaschisis are connected to each other by neurons.
Areas of the brain are connected by vast organized neuronal pathways that allow one area of the brain to influence other areas more farther away from it. Understanding these dense pathways helps to link a lesion causing brain damage in one area of the brain to degeneration in a more distal brain area. So, a focal lesion causes damage that also disturbs the structural and functional connectivity to the brain areas away from the lesion.
This research examined various biochemical aspects of neuroplasticity, specifically, several growth factors. They measured the blood level of brain-derived neurotrophic factor (BDNF), the vascular-endothelial growth factor (VEGF), as well as BDNF RNA gene expression. Additionally, they tested the levels of hepatocyte growth factor, stem cell factor, stromal cell-derived factor 1α, nerve growth factor β, and leukemia inhibitory factor.(2)
They found that PEMF significantly increased growth factors and inflammatory cytokine levels involved in neuroplasticity, as well as promoted an enhancement of functional recovery in post-stroke patients. These effects could be related to the increase of gene expression on the mRNA level. The PEMF group had double the amount of blood serum BDNF and 2.5 times more gene expression. Moreover, increase in BDNF plasma levels was reflected in improvement of the Barthel Index, MMSE, and the opposite with the GDS. They concluded that PEMF therapy improves the effectiveness of rehabilitation of post-stroke patients by improving neuroplasticity processes. PEMF also induced a significant improvement in functional (ADL) and mental (MMSE, GDS) status.
VEGF is involved in the improvement of damaged cells by increasing circulation and restoring function. VEGF levels increased by 50%. The PEMF group also had about 35% better cognitive functioning and 45% better depression scores.
In the non-PEMF group, stroke scale severity and function measures were about 65% and 50% worse, respectively.
The PEMF significantly increased enzyme antioxidant activity. The significant improvements in functional (ADL) and mental (MMSE, GDS) status correlated with the level of enzymatic antioxidant protection. (4)
To determine the level of antioxidant gene expression, they evaluated the level of mRNA expression of catalase, superoxide dismutase, and glutathione peroxidase. After PEMF therapy, mRNA expression of the studied genes (CAT, SOD1, SOD2, GPx1, and GPx4) significantly increased. These changes enhanced the antioxidant defenses of the body. (5)
Apoptosis is programmed cell death, and aims to eliminate damaged cells, including those damaged by the hypoxia of stroke, There are many factors that can induce apoptosis of cells: after ischemia, inflammation, cytokine activation, cascade of free radicals, and induction of thrombin. Neuronal apoptosis is regulated by various genes, such as BCL-2 (inhibitor of apoptosis) and BAX (activator of apoptosis). Induced apoptosis promotes the formation of new neurons, that is, neurogenesis, in mice.
To assess apoptosis gene expression level, (8) these researchers measured the mRNA expression of BAX, BCL-2, CASP8, TNFα, and TP53 in these patients. PEMF significantly increased the expression of BAX, CASP8, TNFα, and TP53, whereas the BCL-2 mRNA expression after PEMF remained similar in both PEMF treatment and control groups. Thus, increasing the expression of pro-apoptotic genes in post-stroke patients promotes the activation of brain neurons and hence brain pathways involved in brain plasticity processes.
Plasma cytokines may be protective (anti-inflammatory) or harmful (pro-inflammatory). The measured the levels of the anti-inflammatory/neuroprotective cytokines interleukin 1β (IL-1β) and transforming growth factor β (TGF-β) and the pro-inflammatory cytokines interleukin 2 (IL-2) and interferon-γ (INF-γ). The level of IL-1β mRNA expression that determines the level of serum IL-1β was also tested. After PEMF treatment, both IL-1β plasma level (up 100%) and IL-1β mRNA expression level (up 70%). On the other hand, IL-2 plasma level increased 15%, while IFN-γ and TGF-β had non-significant changes. The PEMF-induced IL-1β improvement found in this study is likely to have a neuroprotective role. (7)
The researchers also evaluated the possible association between plasma protein oxidative/nitrative damage and the development of poststroke depression. By analyzing several metabolic parameters, they found significant (P < 0.001) differences in all oxidative/nitrative stress parameters in brain stroke patients compared to a healthy group. Oxidative damage of proteins is relates to the degree of poststroke depression. The Geriatric Depression Scale is worse as the concentration of -SH groups or catalase activity increases. (3)
Nitric oxide (NO) is a very important signaling molecule, involved in both physiological and pathological processes. As a neurotransmitter in the central nervous system, NO regulates cerebral blood flow, neurogenesis, and synaptic plasticity. They evaluated the effect of the PEMFs on the generation and metabolism of NO, as a neurotransmitter, in the rehabilitation of poststroke patients. (6) They also measured the levels of 3-nitrotyrosine, nitrate/nitrite, and TNFα in plasma samples, and NOS2 expression in whole blood samples.
PEMF significantly increased 3-nitrotyrosine and nitrate/nitrite levels, while expression of NOS2 was insignificantly decreased in both groups. So, PEMF therapy increases the metabolism and generation of NO, which has both neuroprotective and cytotoxic properties. An increase in NO level is associated with nNOS and/or eNOS activities. It does not influence iNOS expression, which increases mainly during inflammation. Therefore, in the poststroke state, NO demonstrates a protective effect as reflected in significant improvement in functional status.
Direct brain stimulation and timing and age of the patient
Two hundred twenty and three patients with the initial stroke were divided into three groups. (11)
Besides rehabilitation one group was also treated directly to the brain with TMS beginning
from the 6 -10 days after onset, given once a day for 14 days, In another subgroup TMS was begun within 3 months after the initial attack and another subgroup had TMS beginning 3 months after the initial attack. Except for TMS, the basic treatment was the same for all of the patients. Fugl-Meyer score was measured twice: just before treatment and after the 14th treatment.
The effective rate was 91% with TMS plus rehabilitation vs 68% in the control group (P < 0.05).
The Fugl-Meyer scores were 36 and 34 in the rehabilitation subgroup and control subgroup before treatment respectively and were 52 and 40 after treatment respectively (P < 0.01). The Fugl-Meyer scores were 41 and 59 before and after TMS respectively in the subgroup with early TMS treatment (P < 0.01) and were 34 and 45 respectively in the subgroup with TMS beginning 3 months after the onset (P < 0.05).
One of the most widely recognized and clinically relevant measures of body function impairment after stroke is the Fugl-Meyer (FM) assessment. Of the 5 Fugl-Meyer (FM) domains (motor, sensory, balance, range of motion, joint pain), the motor domain, which includes an assessment of the upper extremity (UE) and lower extremity (LE), has well-established reliability and validity as an indicator of motor impairment severity across different stroke recovery time points.
So, what they found was that direct brain TMS is effective in the rehabilitation of motor function in patients with stroke. The effectiveness of TMS treatment depended on the age of the patients and timing of beginning treatment. Results are not as good as people get older and the longer the time treatment is started after the stroke. (11)
Since the Cichon research did not compare different intensities, frequencies, durations of treatment of various PEMF devices or how long after a stroke PEMF should be started, it is not known if there is an optimal PEMF protocol. Because of the very low level of risk in using PEMFs, whether to the pelvic girdle or to the brain, different PEMF protocols may be practical and useful. Both direct brain PEMF stimulation and indirect PEMF stimulation help with recovery from stroke. We will have to wait for studies where they compare indirect stimulation with TMS, to see the levels of effectiveness of each. So, for now, both approaches make sense to help with stroke recovery. Indirect stimulation may be more readily available and able to be used in the home setting at a lower cost.
Benefits of direct brain stimulation with PEMFs
Direct transcranial magnetic stimulation of the brain can induce many of the actions of PEMFs in the body reviewed in the book “Power Tools for Health.” Almost all these actions may be seen with brain stimulation as well. Research shows that TMS can reduce the hyperexcitability seen in pain-related areas of the brain. TMS can trigger spinal cord inhibitory pathways to inhibit the conduction of pain signals to the brain (1). TMS increases cerebral blood flow in affected areas of the brain. In addition, the pain reducing effects of TMS not only influence the endogenous opioid system in the brain but also the endocannabinoid system. TMS can also reduce the neuroinflammation seen after stroke (10), a major contributor to poor stroke outcomes. (12) PEMFs have also been shown to increase neural stem cells useful in brain tissue repair. (9)
CONCLUSION
This research on the use of PEMFs in poststroke recovery and rehabilitation is important in showing some of the mechanisms accounting for the significant benefits from the use of PEMFs seen in those having ischemic strokes, even when applied between 3 to 4 weeks after their stroke. Furthermore, one of the most interesting aspects of this research is the fact that the brain was not even the target of treatment. Even so, peripheral PEMF stimulation appears to be able to provide significant benefits.
It might be expected that more direct treatment to the brain would produce even better results, faster. This research was done using relatively low intensity PEMFs over a short treatment course and short treatment times, ie, 10 PEMF treatments, for 15 mins each, at 5 mT (50 G), 40 Hz. Therefore, the benefits seen in the PEMF treated group were impressive for the amount of treatment effort. Moreover, Even the modified Rankin Scale (mRS), a measure of the degree of disability or dependence in daily activities of people who have suffered a stroke, revealed less disability in those receiving PEMFs.
This is a summary of the results: stroke-related neurological deficit, estimated using NIHSS, decreased approximately 65% more in the PEMF group than in the non-PEMF group. mRS measured disability decreased in both groups, but in the PEMF group the reduction was approximately 50% greater than in the non-PEMF group. About 35% greater improvement was seen in cognitive impairment, as estimated by MMSE, after PEMF treatment. Depressive syndrome, measured in GDS, decreased significantly, with approximately 45% better results in the PEMF group than in the non-PEMF group.
The PEMF treatments used in this study were initiated about 4 weeks after the initial stroke. So, it’s hard to know whether the effects seen of this treatment would have been either earlier or later in the course of recovery from stroke. It is rare to get access to individuals with stroke very early in their disease process, because of the limitations of the complications related to stroke, the hospital environment, the rehabilitation environment and the technology available.
A commonly studied approach to treating stroke is the use of rTMS (repetitive transcranial magnetic stimulation), which uses high intensity PEMFs delivered in highly specialized professional settings. At this point, this therapy is not approved by the FDA or covered by insurance for stroke. Home-based PEMF therapy using medium to high intensity magnetic fields to the brain would be expected to produce good results. This becomes even more feasible when one considers that the PEMF therapy can be started at the home setting, that is, usually after a course of facility-based poststroke rehabilitation. Also, PEMF therapy is not currently
offered in most rehabilitation settings.
Bottom line, PEMF therapies can be a very useful adjunct in the care of people who have suffered strokes, especially when started as soon after stroke as possible, whether the PEMFs are applied directly to the brain or as part of an overall care program. Lastly, whole body PEMF therapy with sufficient intensity PEMF equipment should be used to help the whole person, especially considering that people who have a stroke often multiple health needs that would benefit anyway from PEMF therapy. Lastly.
To determine which PEMF system is best to use specifically for any given person, a free professional consultation is available at https://www.drpawluk.com/consult/
REFERENCES
1. Chang MC, Kwak SG, Park D. The effect of rTMS in the management of pain associated with CRPS. Transl Neurosci. 2020 Sep 28;11(1):363-370.
2. Cichoń N, Bijak M, Czarny P, Miller E, Synowiec E, Sliwinski T, Saluk-Bijak J. Increase in Blood Levels of Growth Factors Involved in the Neuroplasticity Process by Using an Extremely Low Frequency Electromagnetic Field in Post-stroke Patients. Front Aging Neurosci. 2018 Sep
26;10:294.
3. Cichoń N, Bijak M, Miller E, Niwald M, Saluk J. Poststroke depression as a factor adversely affecting the level of oxidative damage to plasma proteins during a brain stroke. Oxid Med Cell Longev. 2015;2015:4
4. Cichoń N, Bijak M, Miller E, Saluk J. Extremely low frequency electromagnetic field (ELF-EMF) reduces oxidative stress and improves functional and psychological status in ischemic stroke patients. Bioelectromagnetics. 2017 Jul;38(5):386-396.
5. Cichon N, Bijak M, Synowiec E, Miller E, Sliwinski T, Saluk-Bijak J. Modulation of antioxidant enzyme gene expression by extremely low frequency electromagnetic field in post-stroke patients. Scand J Clin Lab Invest. 2018 Nov-Dec;78(7-8):626-631.
6. Cichoń N, Czarny P, Bijak M, Miller E, Śliwiński T, Szemraj J, Saluk-Bijak J. Benign Effect of Extremely Low-Frequency Electromagnetic Field on Brain Plasticity Assessed by Nitric Oxide Metabolism during Poststroke Rehabilitation. Oxid Med Cell Longev. 2017;2017:2181942.
7. Cichon N, Saluk-Bijak J, Miller E, Sliwinski T, Synowiec E, Wigner P, Bijak M. Evaluation of the effects of extremely low frequency electromagnetic field on the levels of some inflammatory cytokines in post-stroke patients. J Rehabil Med. 2019 Dec 16;51(11):854-860.
8. Cichon N, Synowiec E, Miller E, Sliwinski T, Ceremuga M, Saluk-Bijak J, Bijak M. Effect of Rehabilitation with Extremely Low Frequency Electromagnetic Field on Molecular Mechanism of Apoptosis in Post-Stroke Patients. Brain Sci. 2020 Apr 30;10(5):266.
9. Cui M, Ge H, Zhao H, Zou Y, Chen Y, Feng H. Electromagnetic Fields for the Regulation of Neural Stem Cells. Stem Cells Int. 2017;2017:9898439.
10. Guo B, Zhang M, Hao W, Wang Y, Zhang T, Liu C. Neuroinflammation mechanisms of neuromodulation therapies for anxiety and depression. Transl Psychiatry. 2023 Jan 9;13(1):5.
11. Jin X, Wu X, Wang J, et al. Effect of transcranial magnetic stimulation on rehabilitation of motor function in patients with cerebral infarction. Zhonghua Yi Xue Za Zhi. 2002 Apr 25;82(8):534-7. Chinese.
12. Jurcau A, Simion A. Neuroinflammation in Cerebral Ischemia and Ischemia/Reperfusion Injuries: From Pathophysiology to Therapeutic Strategies. Int J Mol Sci. 2021 Dec 21;23(1):14.
13. Puderbaugh M, Emmady PD. Neuroplasticity. 2022 May 8. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan–. PMID: 32491743.
PEMF Frequency Needed to Treat Inflammation
Table of Contents
In a previous video, I introduced the idea of the importance of the intensity of the magnetic field needed for magnetic field therapy to give the best results. Furthermore, this video now goes into more detail about the intensity needed to treat inflammation. PEMFs have long been found to help with inflammation and tissue repair and regeneration. Evidently, it is now known that much of this action of PEMFs against inflammation is done by stimulating a molecule in the body called adenosine and its cell adenosine receptors. Consequently, understanding the intensity required for this stimulation is crucial for effective therapy.
PEMFS INCREASE ADENOSINE
Recent PEMF research found that there is an optimum PEMF intensity needed to stimulate the adenosine receptors on the white blood cells. These are the primary immune cells used by the body to combat inflammation. Adenosine is considered the guardian angel of the tissues of the body to protect against runaway inflammation. Moreover, PEMFs increase adenosine throughout the body. Adenosine is needed to produce and release ATP from the mitochondria of cells. ATP is the major source of energy in body tissues. Consequently, as inflammation anywhere in the body increases, a major increase in ATP is needed to control it. In chronic inflammation, the tissues involved often cannot produce enough ATP. Therefore, inflammation persists, damaging tissues and impairing bodily functions.
OPTIMUM PEMF INSTENSITY
So, what is the optimum PEMF intensity required? Firstly, 1.5 mT or 15 Gauss is the optimal intensity at the adenosine receptor on the white blood cell. Therefore, since inflammation can happen anywhere in the body, the starting intensity of the magnetic field required to combat inflammation needs to be considered to give 15 Gauss at whatever depth the tissues are that need treatment. Because magnetic field intensity drops off very rapidly as the field leaves the source of the magnetic field, the intensity of the magnetic field produced has to be considered or calculated based on the depth of the treated tissue.
As an example, if the kidneys are being treated, the depth and the size of the kidneys need to be considered. In an average person, the magnetic field has to achieve 15 Gauss at about 4 inches [10 cm] into the body. That means the starting magnetic field needs to be about 1820 Gauss. Conversely, this same type of calculation needs to be done anytime the body is being treated with a PEMF.
There is a table in a blog on DrPawluk.com that gives these numbers. The blog is called PEMFs, the “guardian angel” adenosine and inflammation. From this table you will know what the starting magnetic field needs to be. It is possible that weaker magnetic fields than optimal may still have value deep in the body, but in my experience, results are less predictable and may take longer, because less adenosine is being produced
Healing with Magnetic Field Therapy
Table of Contents
Board Certified Family Physician and Holistic Health Practitioner. Former Assistant Professor at Johns Hopkins University School of Medicine and University of Maryland. Learn more about his recent talk with Dr. Oz.
Dr. Pawluk is the creator of www.drpawluk.com, an authoritative informational source on PEMFs. He has also authored a book, and appeared and consulted for the media, as well as universities conducting research.
Having healthy cells is not a passive process. Active, regular tuning-up of our cells is not only feasible, but also necessary to slow aging and reduce the risk of cell dysfunction. We are, after all, only as healthy as our cells. Imperceptible cell dysfunction that is not corrected early can lead to disease. Fine-tuning can be done daily in only minutes, using pulsed electromagnetic fields (PEMFs). In addition, when there is a known imbalance (when symptoms are present) or there is a known disease or condition, PEMF treatments, used either alone or along with other therapies, can often help cells rebalance dysfunction faster.
PEMFs work to:
- Reduce pain, inflammation, the effects of stress on the body, and platelet adhesion.
- Improve energy, circulation, blood and tissue oxygenation, sleep quality, blood pressure and cholesterol levels, the uptake of nutrients, cellular detoxification and the ability to regenerate cells.
- Balance the immune system and stimulate RNA and DNA.
- Accelerate repair of bone and soft tissue.
- Relax muscles.
PEMFs have been used extensively for decades for many conditions and medical disciplines, and results can be seen in animals as well as humans. The National Institutes of Health have made PEMFs a priority for research. In fact, many PEMF devices have already been approved by the FDA, some specifically to fuse broken bones, wound healing, pain and tissue swelling, and treat depression. Most therapeutic PEMF devices are considered safe by various standards and organizations.
WHAT ARE PEMFS AND HOW DO THEY WORK?
Science teaches us that everything is energy. Energy is always dynamic and, therefore, has a frequency; it changes by the second or minute, for example, at the very least.
All energy is electromagnetic in nature. All atoms, chemicals and cells produce electromagnetic fields (EMFs). Every organ in thebody produces it own signature bioelectromagnetic field. Science has proven that our bodies actually project their own magnetic fields and that all 70 trillion cells in the body communicate via electromagnetic frequencies. Nothing happens in the body without an electromagnetic exchange. When the electromagnetic activity of the body ceases, life ceases.
Physics, that is, electromagnetic energy, controls chemistry. This in turn controls tissue function. Disruption of electromagnetic energy in cells causes impaired cell metabolism, whatever the initial cause. This happens anywhere in the disease process.
PEMFs address impaired chemistry and thus the function of cells – which in turn, improves health. PEMFs deliver beneficial, health-enhancing EMFs and frequencies to the cells. Low frequency PEMFs of even the weakest strengths pass right through the body, penetrating every cell, tissue, organ and even bone without being absorbed or altered! As they pass through, they stimulate most of the electrical and chemical processes in the tissues. Therapeutic PEMFs are specifically designed to positively support cellular energy, resulting in better cellular health and function.
Devices that produce PEMFs vary by a number of important features: frequency, waveform, strength, and types of stimulators. Frequencies can be simple or complex; and high, medium or low. Intensity can also be high, medium or low.
No “one-size” treatment fits all situations. Most PEMF devices help to varying degrees depending on the problem or condition, but selecting the wrong device may produce unsatisfactory results. Since the body is complex, PEMFs are ideal devices to be able get good results without needing a myriad of different treatments.
AREN’T SOME EMFS BAD FOR YOU?
They can be. Evidence is mounting that a new form of pollution called “electrosmog” is a very real threat because it is disruptive to cell metabolism. Manmade, unnatural EMFs come from electrical wiring and equipment, for example, power lines, communications towers, computers, TVs, cell phones – everything from the wiring in our homes to fluorescent lighting to microwave ovens, hair dryers, clock radios, electric blankets and more.
Electrosmog EMFs are not designed with the body in mind. They can be a strong inducer of stress in the body and, therefore, drain our energy. Electrosmog includes “dirty” electricity, ground currents, microwaves and radio waves. Microwaves are not only from leaky microwave ovens, but also from cell towers, cell phones and wireless equipment.
Electrosmog is all around us and can only be partially blocked. One of the best solutions is to take measures to decrease your exposure. With therapeutic PEMFs, one can purposely add beneficial balancing frequencies to the body to decrease the burden of the negative effects of electrosmog.
PEMFS AND MAGNETS: WHAT’S THE DIFFERENCE?
PEMFs are frequency-based, applied to either the whole body or parts of the body. These PEMFs may only be needed for short periods of time, while the effects last for many hours, setting in motion cellular and whole-body changes to restore and maintain balance in metabolism and health. The body does not acclimate, or “get used to,” the healthy energy signals of therapeutic PEMFs, even if used for a long time, compared to magnets.
Stationary (or “static”), non-varying, magnetic fields from magnets have fixed strengths. They are used in mattresses, bracelets, knee wraps and the like. Most have very shallow penetration into the body, resulting in a very limited ability to affect deeper tissues, and they rarely treat all the cells of the body simultaneously. Only skilled practitioners may guide you to get the bestresults from these approaches.
EXPERIENCE WITH PEMFS
Chiefly, there are quite a number of PEMF systems available now in the US, for daily in-home use, that can help meet your unique needs. Some are FDA-approved and many more are available over-the counter or from various experienced practitioners. Some whole-body systems have been available in the US for over a decade and have been used in Europe by tens of thousands of people for a wide variety of problems without significant negative effects for over 20 years. One PEMF system has been studied through NIH-supported research at the University of Virginia for Rheumatoid Arthritis. These whole body systems have been used worldwide, not only by health-conscious individuals for health improvement and maintenance, but also by world-class and Olympic athletes for increased endurance, enhanced performance, and faster recovery.
WHAT KIND OF DOCTOR CAN HELP ME WITH PEMFS?
Unfortunately, very few conventional, and even alternative or holistic, doctors know about these devices or this technological area. This is not a subject of mandatory education for doctors. Doctors often learn about these new technologies long after the public does, as has been seen with acupuncture. The process of educating doctors and other non-medical practitioners is growing all the time but will take years. Be patient and look for practitioners who have expertise in the area of PEMF therapies.