Painful periods [menses] affect almost 60% of women during adolescence and young adulthood, but may remain until age 50 or menopause. It occurs in 90% of adolescent girls and 50% of women. Most often it begins at the onset of menses or in the first year to 2 years following. Dysmenorrhea is a clustering of symptoms that occurs one to two days before menses, diminishing within two to four days into the flow. These symptoms can include nausea, diarrhea, vomiting, lethargy and headaches, dramatically interfering with daily life for several days a month.
There are 2 types of dysmenorrhea – primary and secondary.
Cause of primary dysmenorrhea
Primary dysmenorrhea usually is caused by the production of natural inflammatory chemicals in the body called prostaglandins. Prostaglandins are made in the lining of the uterus.
Pain usually starts right before menstruation, as the level of progesterone decreases and prostaglandins increase in the lining of the uterus. On the first day of the menstrual period, the levels of prostaglandins are high. The prostaglandins stimulate strong uterine muscle contractions [cramps] which cause decreased blood flow to the uterus and increase pelvic nerve sensitivity that result in sudden increases in pain. As menstruation continues and the lining of the uterus is shed, the levels decrease. Pain usually decreases as the levels of prostaglandins decrease.
Secondary dysmenorrhea
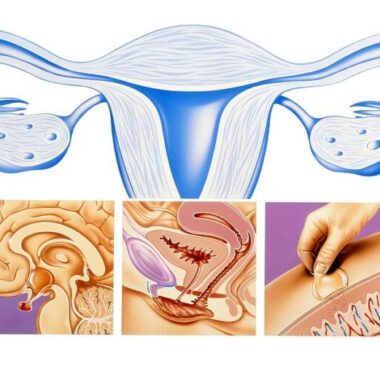
Secondary dysmenorrhea is caused by a disorder in the reproductive system. It usually begins later in life than primary dysmenorrhea. The pain tends to get worse, rather than better, over time. The pain of secondary dysmenorrhea often lasts longer than normal menstrual cramps. It may begin a few days before a menstrual period starts. The pain may get worse as the menstrual period continues and may not go away after it ends.
Some of the conditions that can cause secondary dysmenorrhea include the following:
Endometriosis—In this condition, tissue from the lining of the uterus is found outside the uterus, such as in the ovaries and fallopian tubes, behind the uterus, and on the bladder. Like the lining of the uterus, endometriosis tissue breaks down and bleeds in response to the changes in hormones that happen throughout the menstrual cycle. This bleeding can cause pain, especially right around menstruation. Scar tissue called adhesions may form inside the pelvis where the bleeding occurs. Adhesions can cause organs to stick together, resulting in pain.
Adenomyosis—Tissue that normally lines the uterus begins to grow in the muscle wall of the uterus.
Fibroids—Fibroids are growths that form on the outside, on the inside, or in the walls of the uterus (see the FAQ Uterine Fibroids). Fibroids located in the wall of the uterus can cause pain.
There can be some overlap in symptoms between dysmenorrhea and premenstrual syndrome.
Premenstrual syndrome (PMS) can overlap with dysmenorrhea. PMS symptoms happen between 2 and 12 days before the onset of a period, resolving within the first 24-48 hours of flow. PMS symptoms happen in the phase of the cycle after ovulation.
Treatment of dysmenorrhea
Treatment of dysmenorrhea most typically depends on the use of medications to relieve the pain. These medications, typically nonsteroidal anti-inflammatory drugs [NSAIDS] can cause liver, kidney, blood and gastrointestinal pain, along with nervous system toxicity. A woman taking the maximum dose of NSAIDs throughout her menstrual life increases the risk of kidney damage by 400%.
Hormonal medications, such as birth control pills, often are prescribed. TENS, heat, pelvic floor and aerobic exercises, and acupuncture have been found to have some benefit.
Some lifestyle changes also may help, such as exercise, getting enough sleep, and relaxation techniques. If medications do not relieve pain, treatment will focus on finding and removing the cause of the dysmenorrhea. Surgery may be necessary. In some cases, a mix of treatments works best.
Low level laser therapy [LLLT] can help with symptoms but requires administration by a trained practitioner. Pulsed high-intensity laser therapy [HILT] has also been found useful and needs to be administered professionally.
Efficacy of pulsed electromagnetic fields (PEMFs) in the treatment of primary dysmenorrhea was evaluated in several studies at the same Department of Physical Therapy at Cairo University.
PEMF research for primary dysmenorrhea
Study 1. One study (El-Fatah) applied a 50 Hz, 60 gauss PEMF for one hour only one time on the first day of menstruation to 30 female students, ranging in age from 17 – 25 years. The PEMF was applied with one coil in the area above the upper edge of the pubic bone (suprapubic) and another coil at the same time over the upper lumbar area [T10 – L1]. The mean pain score on a scale from 0 – 4, was 1.77 before starting treatment and 0.27 after treatment. Before treatment 47% had mild pain, 37% moderate, 10% severe and 7% unbearable. After treatment 77% had no pain, 20% had mild pain and 3% had moderate pain. The percentage reduction of pain was 85% (p <.0001).
There was also a significant reduction in symptoms other than pain, from before treatment to after treatment, on the same day.
- Nausea – 73% versus 43%
- Loss of appetite – 90% versus 43%
- Diarrhea – 77% versus 40%
- Water retention – 90% versus 50%
- Dizziness – 77% versus 50%
- Headache – 73% versus 50%
- Mood change – 77% versus 57%
- Psychological symptoms – 100% versus 47%
- Academic productivity – 100% versus 50%
- Social activity – 100% versus 60%
Again, these symptom improvements happened with only one hour of treatment on the first day of menses. More rapid resolution of the symptoms of dysmenorrhea would be expected with daily treatments in the home setting.
The researchers also measured prostaglandin blood levels before and after treatment. The mean levels before and after were 34 versus 13, for a 62% reduction in the blood levels. The reduction in prostaglandin levels even with one hour of stimulation is impressive and likely accounts for much of the benefits seen in reducing the symptoms of dysmenorrhea.
Study 2. Another study (El Refaye) evaluated 50 adult female university students. They compared use of PEMFs with the use of an NSAID (diclofenac). The PEMF was applied for 20 minutes to the pelvic area three times per cycle for three consecutive cycles. The applications were before the onset of menstrual flow, then the first and second days after flow began. For three consecutive cycles. The NSAID group received 50 mg of diclofenac once only at the onset of menstrual pain for three consecutive cycles. They had measurements of pain levels, physical and psychological symptoms and blood progesterone levels. The PEMF device was 60 Gauss at 50 Hz. As in the previous study the coils were applied to the suprapubic area and over the lumbar spine (T10-L1). Pain and progesterone levels were measured before treatment and after the third cycle.
Progesterone was measured because progesterone inhibits prostaglandin production in the uterus, blocks the action of prostaglandin and increases its inactivation rate. Therefore, increasing progesterone production or availability decreases uterine muscle contractions. This is also why many doctors prescribe progesterone pills to control dysmenorrhea.
From before to after treatment, in the PEMF group, the progesterone level increased by 184%, the pain level decreased by 67% and the menstrual symptom score improved by 41%. In the NSAID/diclofenac group, the progesterone level barely changed, the pain level only decreased by 50% and the menstrual symptom score improved only by 27%. When these results were compared between the groups statistically, the PEMF treatment group did significantly better than the diclofenac group.
Study 3. A third study (Thabet) compared the use of high intensity laser therapy (HILT) to PEMF therapy. Fifty-two women between ages 18 – 24 with primary dysmenorrhea were recruited to be evaluated. As with the other studies, the PEMF was 50 Hz and 60 gauss. The coils were applied to the suprapubic area and the lower back (L4-S3) for 30 minutes, three times per cycle for three consecutive cycles. The applications were done before the onset of menstrual flow, then the first and second days after flow began. In this study they measured current pain, pain relief and prostaglandin (PG) levels. Pain was measured before and right after the last – third treatment. The PG level was measured before and three months after treatment.
HILT was administered by a trained professional using a very expensive professional grade laser system. The laser was applied in three phases, to multiple locations, for over 15 minutes of application time, at each treatment session.
The before and after pain scores for the laser system were a mean of 3.2 vs 0.7 for a 78% improvement. The before and after pain scores for the PEMF system were 3.3 versus 1.2 for a 62% improvement. Statistically speaking, the laser treatment produced more benefit. The average pain relief scores for the laser group was 3.2 versus 2.7 for the PEMF group. As far as prostaglandin level changes, the mean difference for HILT was 19.4 versus 17.64 for PEMFs, with comparable 59% and 54% improvements, respectively.
Bottom line for this study is that both treatment methods have significant reductions in pain severity and prostaglandin levels. HILT therapy was somewhat more effective than the particular PEMF therapy used. The contrast is that HILT requires very expensive equipment, significant time and effort, including disrobing, professional treatment and all the associated costs. Neither treatment is anticipated to produce long-term benefits, so recurring treatments are likely necessary. PEMFs would be the most cost-effective.
Conclusion
Dysmenorrhea is a very burdensome problem that happens to women through their menstrual life, usually for years. There is still a great unmet need to reduce the personal burden of coping with days of disabling and disruptive symptoms, loss of productivity, psychological effects and the potential risks associated with treatments. Even a 60 Gauss magnetic field, applied for short periods of time can produce significant symptom reduction. The mechanisms for the benefit are multiple and at the very least include increasing progesterone levels and decreasing prostaglandin production, prostaglandins being the source of most of the symptoms.
While the research reviewed deals primarily with primary dysmenorrhea, PEMFs have been shown to be helpful for other forms of secondary dysmenorrhea, especially for endometriosis and also for pelvic pain issues in general, not to mention countless other uses.
It is recommended that women who have this issue should have for their personal use a portable battery-operated PEMF system that can be used just before a period begins and for the several days that symptoms last. Once owned, this type of PEMF system may be useful for many other symptoms and health issues for which PEMFs have been shown to be beneficial.
Higher intensity PEMF systems may be even more beneficial than the intensities used in the studies reviewed above. As a result, treatment times may be able to be shorter for any given treatment session and used for fewer days through a cycle. Dysmenorrhea includes significant inflammation and pain. There is more discussion about reducing inflammation and pain through effects on the adenosine receptor, which is also present in the uterus.
See the book Power Tools for Health: How Pulsed Magnetic Fields (PEMFs) Help You.
References
El Refaye GE, Botla AM, Hussein HAD, et al. Electromagnetic field versus diclofenac drugs on primary dysmenorrhea: A single-blind randomized controlled trial. J Clin Analytical Med. 2019 Mar;10(2): 202-206.
Thabet AAE, Elsodany AM, Battecha KH, et al. High-intensity laser therapy versus pulsed electromagnetic field in the treatment of primary dysmenorrhea. J Phys Ther Sci. 2017 Oct;29(10):1742-1748.